Top Topics
Thank you for your quick reply and explanation. That makes sense. Following your message, I was actually able to get much better agreement in the CCSHS dataset by linking hypopnea events with SpO2 desat and/or arousals. This approach doesn't work as well in the SHHS dataset (and MESA to some extent) unfortunately — most likely because of the known issues of the XML annotations — but it still gives better overall agreement.
Hi,
This is somewhat related to this post.
I am not able to re-calculate the AHI reported in ccshs-trec-harmonized-0.7.0.csv from the XML annotation files. For example, night ccshs-trec-1800001 has 17 Hypopnea and 1 Central Apnea in the XML file, i.e. a total of 18 events. The total sleep time (ttldursp_f1) is 490 minutes. The AHI should be 60 * 18 / 490 = 2.20 events / hour. However,the AHI values are much lower in ccshs-trec-harmonized-0.7.0.csv, regardless of the definition: 0.24 for ahi_hp3u, 0.24 for ahi_hp3r_aasm15 and 0.12 for ahi_hp4r.
ttldursp_f1
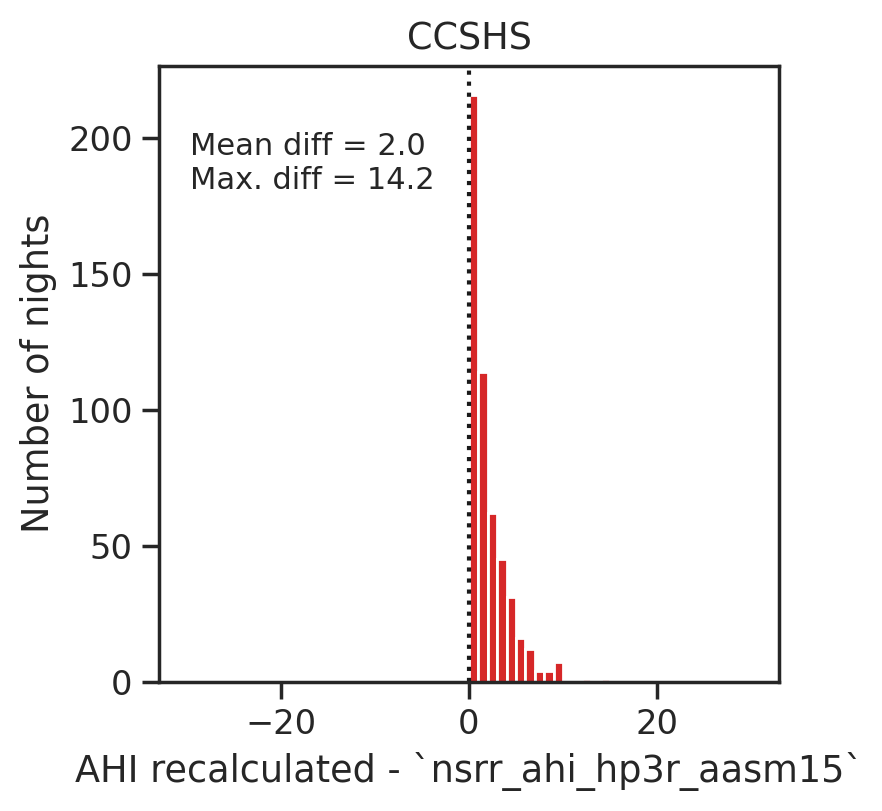
I looked at the entire CCSHS dataset and you can see that on average the manually-recalculated AHI is 2 events / hour higher than ahi_hp3r_aasm15:
I also looked at the MESA and SHHS dataset and have found the same issue, even when excluding events that were scored during wake periods. For example, in MESA the recalculated AHI is on average 10 events / hour higher than the AHI in the main CSV file.
Am I missing something? Is there any additional filtering of the XML events required to get closer to the true AHI?
Thanks for your help, Raphael